
Your cart
There are no more items in your cart








{kind=link}
{kind=link}
{kind=link}
Made in ultra-high resolution 3D printing in full color.
Pionephrosis - Erler Zimmer 3D anatomy Series MP2096
This dissection model highlighting Pionephrosis is part of the exclusive Monash 3D anatomy series, a comprehensive series of human dissections reproduced with ultra-high resolution color 3D printing.
Clinical history
A 38-year-old woman presents with severe nausea, vomiting, fevers, and chills. She has a history of recurrent urinary tract infections in the past 6 months. She has required several courses of oral antibiotics and a hospitalization for IV antibiotics. Blood tests show increased inflammatory markers. Urinalysis is positive for white blood cells (WBC). A CT scan shows unilateral left hydronephrosis and pyelonephritis. She does not respond to conservative treatment and undergoes nephrectomy. She makes a full recovery.
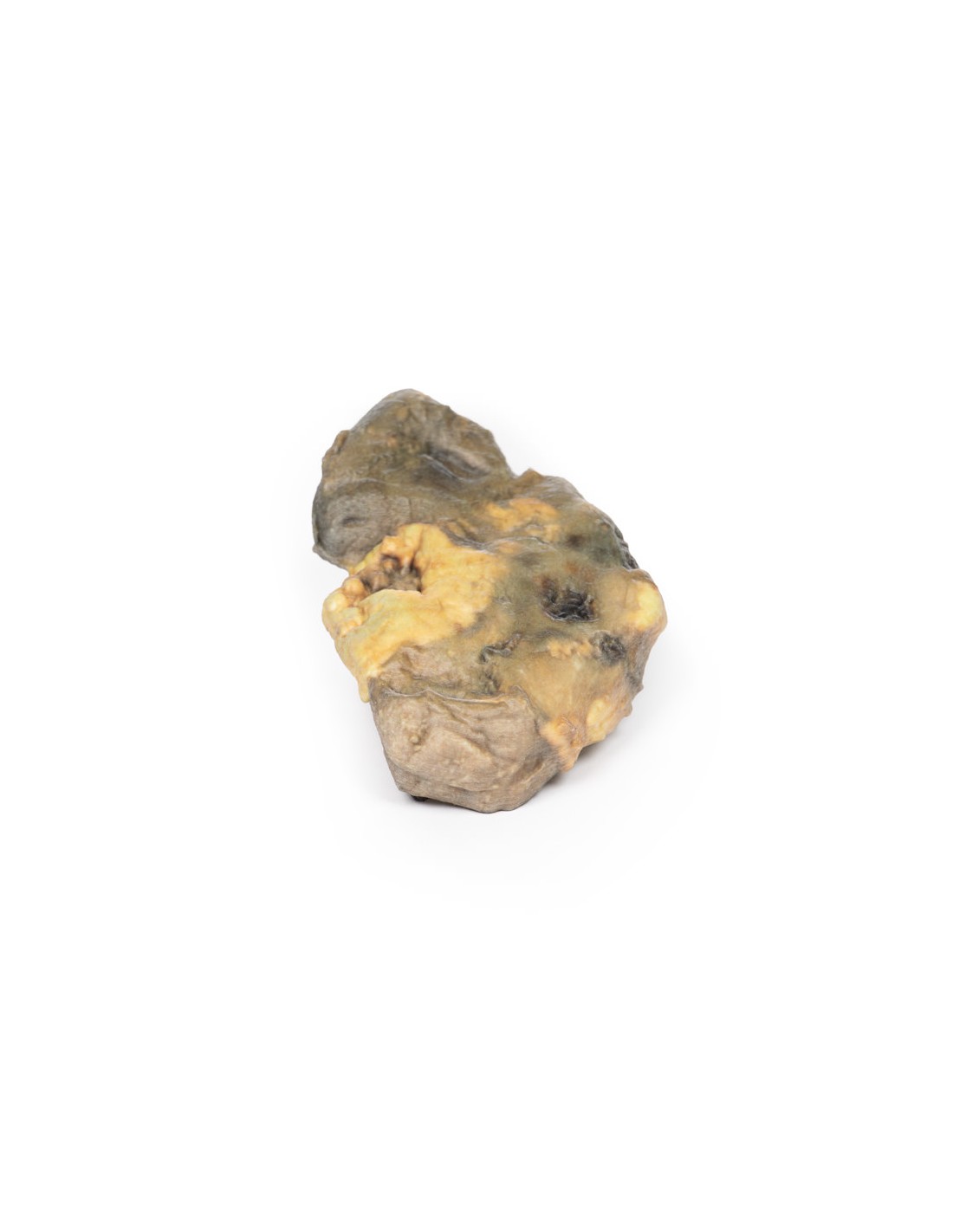
Pathology
This is the patient's left nephrectomy specimen. The kidney has been sliced to show the cut surface. The pelvis and calyces are greatly dilated and contain remnants of yellow pus. There is considerable fibrosis of the renal parenchyma. In the median area near the lateral border there is a necrotic hemorrhagic area 35 x 12 mm in diameter containing pus. Two similar small hemorrhagic necrotic areas are visible on the capsular surface. These lesions are probably continuous with the lesion observed on the cut surface, probably caused by hemorrhage into an abscess cavity. This lesion would have resulted in a perinephric abscess.
Further information
Pyonephrosis occurs when there is obstruction within the upper urinary tract and pyelonephritis. Debris from the infection, white blood cells and bacteria accumulate in the obstructed kidney, resulting in a pus-filled hydronephrotic kidney. A staghorn stone usually forms in association with a chronic or recurrent infection as a result of the more alkaline urinary pH caused by the bacterial infection.
Pyonephrosis is a rare condition. Risk factors for development include immunosuppression, diabetes, and anatomic obstructions of the urinary tract, e.g., urinary tract stenosis, horseshoe kidneys, tumors, urinary stones. The clinical presentation may consist of vague symptoms, but may include constitutional symptoms of sepsis, flank pain, hematuria, dysuria, and pyuria. A grossly nephrotic kidney may be palpable on palpation of the abdomen. Pyuria will be present on urinalysis. Radiologic diagnosis can be made usually using CT investigations but also ultrasonography or MRI looking for evidence of urinary tract obstruction and pyelonephritis.
Treatment will depend on the cause of the obstructive lesion. Emergent treatment involves drainage of the purulent accumulation within the kidney. This is performed by urology or interventional radiologists via percutaneous or retrograde ureteral stents to relieve the obstruction and drain the pus. Further surgical treatment will depend on the cause of the obstruction. Antibiotic therapy is necessary to treat the underlying infection or sepsis. If complications such as florid sepsis, xanthogranulomatous pyelonephritis, renal or perinephric abscess formation, or fistulae in the pleura, colon, or duodenum are not treated.
.
What advantages does the Monash University anatomical dissection collection offer over plastic models or plastinated human specimens?
- Each body replica has been carefully created from selected patient X-ray data or human cadaver specimens selected by a highly trained team of anatomists at the Monash University Center for Human Anatomy Education to illustrate a range of clinically important areas of anatomy with a quality and fidelity that cannot be achieved with conventional anatomical models-this is real anatomy, not stylized anatomy.
- Each body replica has been rigorously checked by a team of highly trained anatomists at the Center for Human Anatomy Education, Monash University, to ensure the anatomical accuracy of the final product.
- The body replicas are not real human tissue and therefore not subject to any barriers of transportation, import, or use in educational facilities that do not hold an anatomy license. The Monash 3D Anatomy dissection series avoids these and other ethical issues that are raised when dealing with plastinated human remains.
No reviews
Tap to zoom
